
The Invisible Exposure - What the Science Actually Says About EMF and 5G |
The mounting evidence for electromagnetic field dangers and what the telecommunications industry doesn't want discussed |
We live in an invisible sea of electromagnetic radiation. From the Wi-Fi router in your home to the cell tower down the street, from your smartphone to the 5G infrastructure now being deployed across cities worldwide, most people in developed countries are now exposed to artificial electromagnetic fields (EMFs) almost continuously.
The question of what that exposure does to the human body has generated serious scientific debate for decades. The answers are considerably more complicated than either the telecommunications industry or many health advocates suggest.
This article examines the peer-reviewed evidence, explains how safety standards are set and where their limits lie, and offers a practical framework for navigating a genuinely contested area of science (at least if you include all the industry funded studies).
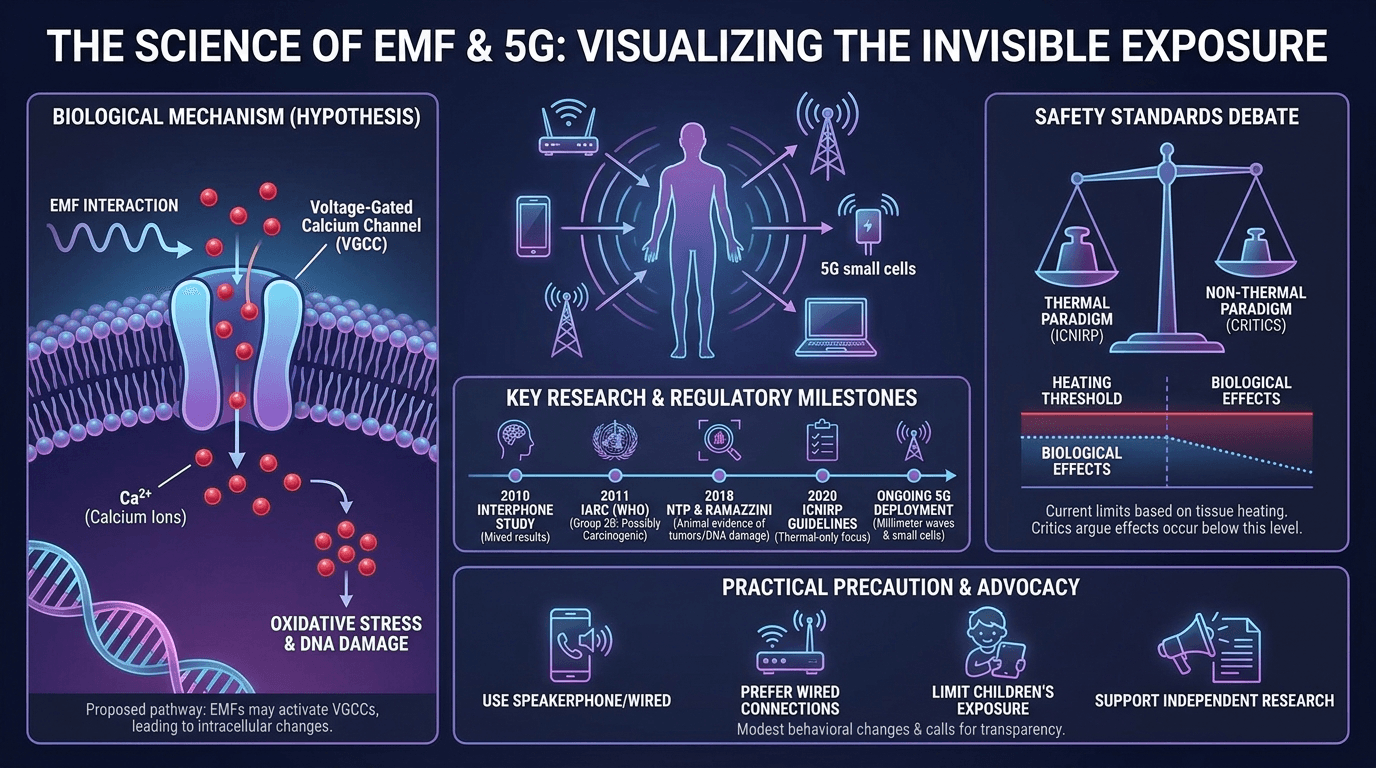
The Biological Mechanism: How EMFs Interact with Cells
The most specific scientific hypothesis for how non-ionising EMF exposure could affect biology centers on voltage-gated calcium channels (VGCCs). These protein structures sit within cell membranes and control the flow of calcium ions into cells.
Calcium signaling governs nearly every cellular process: muscle contraction, nerve impulse transmission, hormone secretion, and gene expression all depend on precise calcium dynamics.
Dr Martin Pall, Professor Emeritus of Biochemistry and Basic Medical Sciences at Washington State University, proposed in a 2013 review that EMFs interact with the voltage sensor on VGCCs, causing them to open when they should not. The result is an abnormal influx of calcium, triggering a cascade that produces peroxynitrite, a reactive compound that causes oxidative stress and DNA strand breaks.
Pall's paper, published in the Journal of Cellular and Molecular Medicine, reviewed 23 studies supporting this mechanism and noted that VGCC blockers inhibit these EMF effects, which he argues constitutes pharmacological evidence for the pathway [1].
VGCCs are concentrated in the nervous system and heart, which may explain why reported symptoms in EMF-sensitive individuals commonly involve the brain and cardiovascular system. The mechanism is biologically plausible but contested (mostly by industry funded shills if you actually dig into funding).
Critics argue the energy levels in non-ionising radiation are far too low to force ion channels open under controlled conditions. Wishful thinking considering these effects have been documented for many years.
This debate between thermal and non-thermal effects sits at the heart of the regulatory dispute. Current safety standards in the US are built on the thermal model alone: the idea that non-ionizing radiation can only harm by heating tissue, and that no biological effects occur below that threshold.
The non-thermal paradigm, supported by Pall and others, holds that biological effects occur at intensities thousands of times below the heating threshold. Many countries have updated their thresholds of safety far below the ancient 1996 guidelines still followed in the agency captured US regulatory region.
What the Research Shows: Tumor Studies and Regulatory MilestonesThe IARC 2B Classification
The most significant official acknowledgment that RF-EMF warrants concern came in May 2011. The International Agency for Research on Cancer (IARC), a branch of the WHO, convened a working group of 31 scientists from 14 countries. Their conclusion: radiofrequency electromagnetic fields are "possibly carcinogenic to humans," placing them in Group 2B on the IARC scale [2].
The classification was based primarily on evidence of increased glioma risk in heavy mobile phone users.
Group 2B is the weakest positive finding in IARC's system: it means limited evidence in humans and limited or inadequate evidence in animals. For context, coffee and talc-based body powder carry the same classification. Group 2B is not a finding of harm; it is a formal signal that the global regulatory body for cancer research considers the question open. It's representative of how slow the ball moves in the captured regulatory systems on RF radiation.
Is this proof that the regulatory agencies are owned by the industry they regulate? I'll let you make your own conclusion on that.
The Interphone Study
The primary epidemiological study informing the IARC decision was the Interphone study: a WHO-coordinated case-control study spanning 13 countries, published in the International Journal of Epidemiology in 2010 [3].
Over 5,000 glioma and meningioma cases were recruited alongside matched controls, making it one of the largest brain tumor studies ever conducted.
Results were mixed. Overall, regular mobile phone users showed no increased glioma risk; the odds ratio was slightly reduced, attributed to participation bias. However, in the highest group of cumulative call time (over 1,640 hours total), there was a non-significant increased odds ratio for ipsilateral glioma. The authors acknowledged the study's inability to capture long latency periods.
The Hardell Research Program
Swedish oncologist Lennart Hardell of Orebro University Hospital has published extensive epidemiological research on mobile phone use and brain tumors.
A 2017 analysis by Carlberg and Hardell applied Bradford Hill's causation criteria to the accumulated evidence and found an odds ratio of 1.90 (95% CI: 1.31-2.76) for glioma in the highest cumulative exposure group [4], rising to 2.01 for those with more than 20 years of wireless phone use.
Swedish data also indicate that people who begin using mobile or cordless phones before age 20 face more than a fourfold increased ipsilateral glioma risk, possibly because younger skulls are thinner and developing brains may be more susceptible [5].
These findings represent the more alarming end of the published spectrum; other groups working with the same populations have reached less alarming conclusions. However, Hardell's work is peer-reviewed and cannot be dismissed simply because it is inconvenient.
The NTP and Ramazzini Animal Studies
Two large-scale animal studies published in 2018 added a different kind of evidence.
The US National Toxicology Program (NTP) conducted two-year studies in rats and mice exposed to radiofrequency radiation at levels used by 2G and 3G mobile phones [6].
Published in November 2018, the findings showed "clear evidence" of an association between high RFR exposure and malignant schwannomas in the hearts of male rats, and "some evidence" of malignant gliomas in male rat brains. NTP scientists also found RFR exposure linked with DNA damage in the frontal cortex and hippocampus. These were high-exposure studies, and critics note the doses were calibrated to the upper end of human device-level exposure, not ambient levels.
That being said, how much more radiation do you think the younger generations have been exposed to since the time of this study? Newer phones and higher background radiation levels represent huge increases of exposure that likely are even higher than these original NTP scientists were explosing.
Complementing the NTP work, the Ramazzini Institute in Italy used far lower exposure levels representative of base station environmental emissions [7].
Despite the lower intensities, Ramazzini rats showed an increased incidence of heart schwannomas consistent with the NTP findings, a result that matters because NTP's critics had argued its results were only relevant at unrealistically high doses.
5G: New Technology, Familiar Regulatory Gaps
5G is not simply a faster version of 4G. It introduces new frequency bands, including millimeter wave frequencies (24-100 GHz) in some cases, not previously used in consumer telecommunications.
Because millimeter waves do not travel far and are absorbed easily by obstacles, 5G networks require denser infrastructure of small cells closer to where people live and work.
The health question around millimeter waves differs from that around sub-6 GHz frequencies. At these higher frequencies, radiation penetrates only the outer layers of skin and the surface of the eyes rather than deeper tissues.
Long-term peer-reviewed data on chronic low-level millimeter wave exposure in humans does not yet exist. The 2020 ICNIRP guidelines cover the full range up to 300 GHz and set limits based on a maximum temperature rise of 2 degrees Celsius in the skin, maintaining the thermal-effects-only framework.
Pall's 2021 paper in Reviews on Environmental Health argues that millimeter waves may activate VGCCs in skin and corneal cells, and that the non-penetration assumption ignores indirect effects through nerve fibers in the skin [8]. This remains disputed by mainstream bioelectromagnetics bodies, largely industry funded shills in the opinion of the author.
In 2017, more than 400 scientists and medical doctors signed the 5G Appeal to the European Commission, calling for a moratorium on 5G roll-out pending independent safety review. The appeal did not produce a moratorium but remains a documented expression of concern from within the scientific community.
Electromagnetic Hypersensitivity: Real Condition, Contested Cause
Electromagnetic hypersensitivity (EHS) refers to a cluster of non-specific symptoms attributed by affected individuals to EMF exposure: headaches, fatigue, concentration difficulties, dizziness, and heart palpitations. These symptoms are real and can be severely disabling for a significant minority.
The WHO's fact sheet on EHS is careful to separate the symptoms from their cause. The WHO acknowledges that EHS symptoms are "certainly real and can vary widely in their severity," but is equally clear that "there is no scientific basis to link EHS symptoms to EMF exposure" [9].
Double-blind provocation studies consistently show that symptom onset does not correlate with actual EMF levels. EHS is not a recognised medical diagnosis but anyone in the health field that is actually paying attention to metabolic health is keenly aware of the seriousness of EHS and it's clear association with EMF/RFR exposure.
The WHO notes that reported EHS prevalence varies considerably across countries, with higher rates in Sweden, Germany, and Denmark. Population surveys in Europe have estimated somewhere between 1.5% and 10% of people self-reporting EHS-like symptoms, depending on country and definition.
The original article's claim of "3-5% severe, up to 30% mild" could not be traced to a peer-reviewed source and is not used here. Physicians are advised by the WHO to focus on the health symptoms and clinical picture rather than the patient's attribution of those symptoms to EMF. This approach neglects the serious implications of EMF hypersensitivity, representing the gaslighting of real symptoms and the convenience of brushing them under the rug instead of truly addressing people affected by EHS.
How Safety Standards Are Set: The Thermal Paradigm and Its Critics
The standards governing public RF-EMF exposure in most countries derive from guidelines produced by the International Commission on Non-Ionizing Radiation Protection (ICNIRP), a private scientific body registered in Germany. ICNIRP's guidelines were updated in 2020, covering 100 kHz to 300 GHz [10], and are adopted by the EU and used as the basis for limits in many other countries. The FCC in the United States uses similar guidelines, last substantially updated in the 1990s, likely due to regulatory capture which prefers to ignore the new published science.
ICNIRP establishes limits based on the level required to prevent tissue heating beyond a defined threshold. The 2020 guidelines set a whole-body average SAR of 0.4 W/kg for workers and 2 W/kg (averaged over 10g of tissue) for the general public.
The central criticism: these limits only account for thermal effects, not biological changes below the heating threshold. Critics also note that ICNIRP is a private self-selecting committee with no governmental mandate. ICNIRP responds that there is no reliably replicated evidence of adverse effects below thermal thresholds, and that the 2020 guidelines incorporated a systematic review of thousands of papers. They conveniently ignore all the VGCC activation research highlighted by Pall and others.
The BioInitiative Report, updated from its 2012 base, argues that existing standards are inadequate and that evidence exists for increased cancer risk and neurological effects at levels far below current guidelines [11]. It is not a peer-reviewed publication: it is an advocacy document by researchers who favor precautionary limits, and it functions as a curated argument rather than a balanced literature review. Children and Vulnerable Populations
One area of greater scientific agreement concerns differential risk for children. Younger skulls are thinner, developing brains may be more susceptible to external influences, and today's children begin using mobile devices far earlier than the first generation of wireless users studied.
The Davis et al. 2013 review of Swedish data found that individuals who began mobile phone use before age 20 had more than a fourfold increased risk of ipsilateral glioma compared with non-users [5].
Several health bodies, including France's ANSES, have recommended precautionary measures specifically for children, including limiting mobile phone use and mandating hands-free kits. This does not require accepting the strongest version of the non-thermal hypothesis. Even accepting only the IARC 2B classification, the implications for children (who will accumulate far more lifetime exposure than current adult users) are a reasonable basis for precautionary guidance.
What You Can Do
The honest position if you believe all the industry funded studies is that the evidence base is genuinely uncertain, but when taking into account where funding for various studies comes from a different conclusion emerges.
The IARC classification, the NTP and Ramazzini animal studies, Hardell's epidemiological work and Pall's VGCC work together represent a body of evidence that regulators should take more seriously than current standards reflect. While this evidence may not prove that mobile phones cause cancer at population level, it sure does indicate that it's a contributing factor to take note of and is significant enough to revise exposure limits, especially noting the significant regulatory capture in US and International regulatory agencies.
After all, when the fox is guarding the hen-house what do you actually expect to happen?
Practical precaution is reasonable, particularly given that the cost of modest behavioral changes is low.
For personal exposure:
At a systemic level:
Conclusion
The science of EMF and health does not divide neatly into "harmful" and "safe." There is enough evidence of biological effects, and enough uncertainty about long-term consequences, to take the question seriously and question the threshold levels set by regulatory bodies due to their conflicts of interest with the revolving door of regulators that guard the henhouse.
It is clear is that the regulatory framework has not kept pace with the technology it governs. Safety limits based on tissue heating, set by a private body using 1990s-era assumptions, now apply to millimeter wave frequencies that did not exist in consumer products when those limits were written and exposure levels not seen with 1990's devices.
The telecommunications industry's pattern of funding research that finds no effect, paralleled by independent research consistently finding biological signals, follows a trajectory that should give pause: not because conspiracy is the only explanation, but because it is a well-documented pattern in the history of industrial health science.
Precaution, where the cost of caution is low and the potential downside is serious, is not alarmism. It is basic prudence.
What do you think? Share your thoughts below.
References
|

5 Comments
Join the conversation
The NTP rat study findings were interesting but worth noting those animals were exposed to far higher levels than typical phone users. Extrapolating that directly to humans scrolling instagram is a stretch. Not saying there's nothing here, just that the framing glosses over some pretty significant caveats.
Maybe far higher levels than exposure was in 2012 but is that really lower than what we are exposed to now with so much background radiation?
Been using speakerphone for calls for years now, mostly because it's just easier, but good to know there might actually be a reason beyond convenience. The airtube earpiece thing is new to me though, had no idea that was a thing.
The EHS section is so important. I know someone who had to basically rebuild her whole life around avoiding wifi and people treated her like she was making it up. Whether or not the mechanism is proven, the suffering is real. Glad to see it at least acknowledged here.
The part about children and thinner skulls really got me. My kids have had tablets since they were toddlers and I never once thought to question it. Going to start keeping the router out of their rooms at least. Small change but feels worth it.