
Amygdalin's Anticancer Mechanisms: What the Research Actually Shows |
Enter Subtitle |
The medical establishment wants you to believe that amygdalin is nothing more than dangerous quackery peddled by desperate patients and opportunistic charlatans. But they don't tell you about the growing body of peer-reviewed research showing precisely how this compound triggers cancer cell death while leaving healthy cells largely untouched. They don't mention the molecular pathways, the enzymatic mechanisms, or the cancer types responding when conventional therapies have failed.
After all, if a natural compound can do what billion-dollar chemotherapy drugs promise - but can't always deliver - where does that leave the cancer-industrial complex? Where does it leave the pharmaceutical companies that can't patent nature's molecules?
The Apoptosis Pathway: Flipping Nature's Death Switch
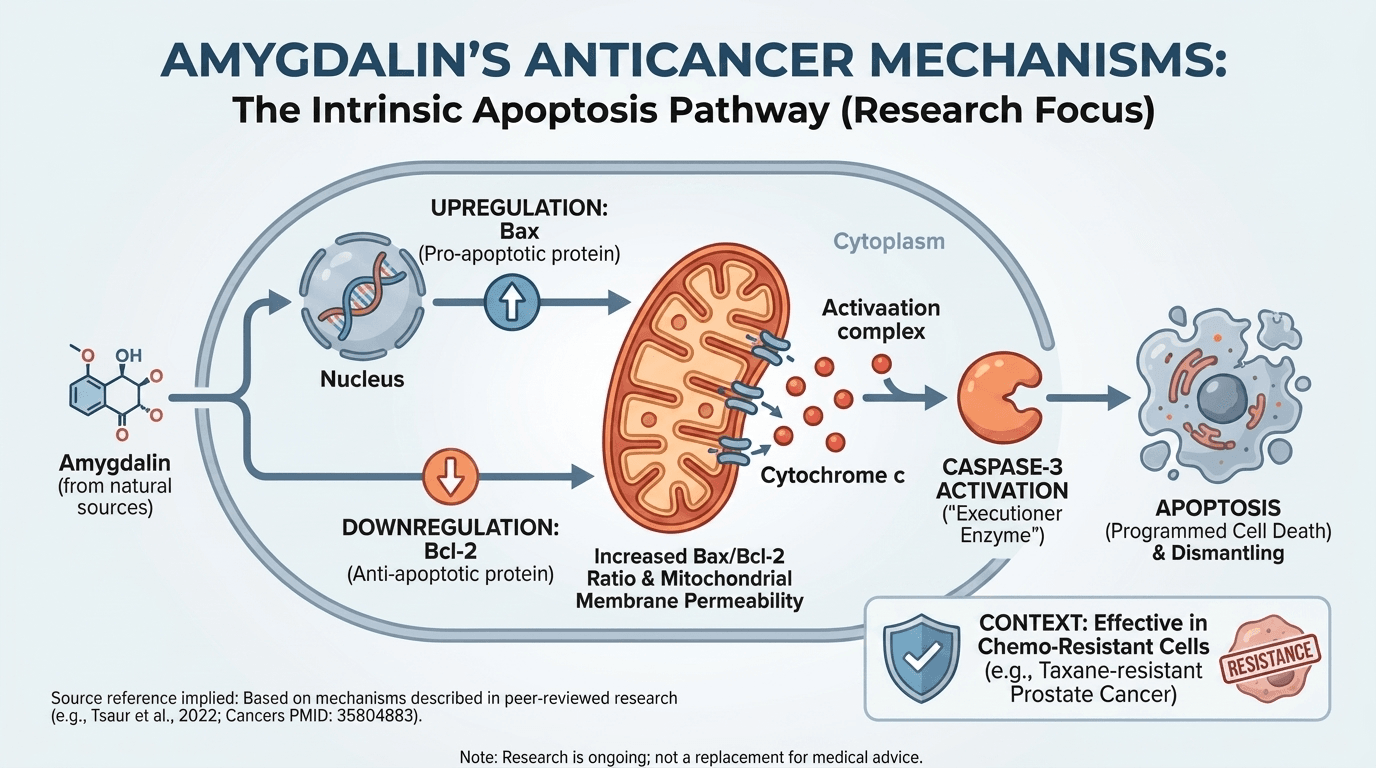
Cancer cells are essentially immortal - they've disabled their own suicide programs through mutations in apoptosis regulatory genes. This cellular immortality is a hallmark of malignancy. Amygdalin, according to researchers like Tsaur and colleagues (2022), appears to flip that death switch back on, restoring the cell's ability to recognize when it should die.
Their groundbreaking work on taxane-resistant prostate cancer cells revealed something the oncology establishment doesn't want acknowledged: amygdalin activated caspase-3, the executioner enzyme that systematically dismantles cells from within during programmed cell death (Cancers, PMID: 35804883). Keep in mind, these were PC-3 and DU145 cancer cell lines that had already developed resistance to docetaxel and cabazitaxel - frontline chemotherapy agents. The drugs had failed. Resistance mechanisms were fully operational. But amygdalin triggered the death cascade anyway.
The mechanism involves upregulation of Bax (a pro-apoptotic Bcl-2 family protein that makes mitochondrial membranes permeable) and downregulation of Bcl-2 (an anti-apoptotic protein that prevents mitochondrial membrane disruption). In plain language: amygdalin tells cancer cells to die and simultaneously removes the molecular brakes preventing their death. It's a two-pronged attack on cancer cell survival.
Additionally, amygdalin treatment increased the Bax/Bcl-2 ratio - a critical determinant of whether cells proceed with apoptosis. When this ratio tips in favor of Bax, mitochondria release cytochrome c into the cytoplasm, triggering the caspase cascade. This is the intrinsic apoptosis pathway, and amygdalin appears to activate it selectively in malignant cells.
Cell Cycle Arrest: Stopping Cancer in Its Tracks
Cancer's defining feature is uncontrolled proliferation - cells dividing without restraint, ignoring normal regulatory checkpoints. Amygdalin interrupts this process by arresting cells at specific checkpoints in their division cycle, preventing them from completing DNA replication and mitosis.
Spanoudaki et al. (2023) documented cell cycle arrest at the G0/G1 phase in multiple cancer cell lines (Int J Mol Sci, PMID: 37762572). Translation: cancer cells get stuck before they can replicate their DNA and divide. The relentless growth engine grinds to a halt.
The mechanism involves reduction of cyclin A and CDK2 (cyclin-dependent kinase 2), as demonstrated by Makarević et al. (2014) in bladder cancer cells (PMID: 25136960). Cyclin A/CDK2 complexes are essential for S-phase entry - when DNA replication occurs. Without functional cyclin A/CDK2, cells cannot progress through the cycle. They accumulate in G1, unable to advance, and eventually undergo apoptosis or senescence.
Here's the rub: normal cells can often recover from this arrest when the stressor is removed. They have intact checkpoint machinery and can resume normal cycling. Cancer cells, already stressed and metabolically compromised, often cannot. The selectivity isn't perfect - no cancer treatment achieves perfect selectivity - but the differential vulnerability exists and is measurable.
The Beta-Glucosidase Differential: Selective Activation
Critics fixate obsessively on cyanide toxicity, as if amygdalin circulates through the body indiscriminately releasing poison. Proponents point to cancer cells' enzymatic vulnerabilities - the biochemical Achilles' heel that makes selective toxicity possible.
Cancer cells produce significantly higher levels of beta-glucosidase - the enzyme that cleaves amygdalin's glycosidic bonds, releasing hydrogen cyanide - and lower levels of rhodanese (thiosulfate sulfurtransferase), the mitochondrial enzyme that detoxifies cyanide by converting it to thiocyanate. Barakat et al. (2022) reviewed the biochemical rationale extensively: cancer cells essentially poison themselves when exposed to amygdalin (PMC9599719).
Normal cells, rich in rhodanese and deficient in beta-glucosidase, can neutralize the small amounts of hydrogen cyanide released during amygdalin metabolism. They possess the enzymatic machinery to convert HCN to harmless thiocyanate, which is then excreted renally. It's a biochemical trap that exploits the metabolic abnormalities of cancer cells - a targeted kill mechanism encoded in enzymatic differences.
After all, this isn't theoretical speculation. Cipollone et al. (2008) documented the critical role of rhodanese in cyanide detoxification, demonstrating that this enzyme is the primary defense mechanism against cyanogenic compounds (J Mol Microbiol Biotechnol, PMID: 18685272). Cancer cells' relative rhodanese deficiency makes them vulnerable to amygdalin's cyanide-releasing mechanism.
Which Cancers Have Been Studied? The Evidence Base
The research spans multiple cancer types, far more than the mainstream medical narrative acknowledges:
Prostate Cancer: Tsaur's landmark 2022 study showed efficacy against taxane-resistant PC-3 and DU145 cell lines - aggressive castration-resistant prostate cancers where conventional therapy has exhausted options. Amygdalin induced apoptosis, reduced cell viability, and overcame taxane resistance mechanisms. This isn't treating early-stage disease; this is salvaging cases where everything else has failed.
Breast Cancer: Abdel-Mageid et al. (2025) demonstrated protective and chemotherapeutic effects in mammary cancer models (Sci Rep). Amygdalin treatment resulted in measurable tumor regression and upregulation of critical tumor suppressor genes including p53 (the "guardian of the genome") and BRCA1 (involved in DNA repair). The compound didn't just kill cancer cells - it restored expression of genes that prevent cancer from developing in the first place.
Bladder Cancer: Makarević et al. (2014) demonstrated dual mechanisms: cell cycle arrest via cyclin A/CDK2 reduction (PMID: 25333694) and reduced adhesion/invasion (PMID: 25333694). The latter finding is particularly significant - metastasis, not primary tumors, is what kills most cancer patients. Amygdalin appears to interfere with cancer cells' ability to detach, migrate, and invade distant tissues.
Notably, Syrigos et al. (1998) pioneered targeted delivery by conjugating beta-glucosidase to a bladder cancer-associated monoclonal antibody (HMFG1), demonstrating enhanced cytotoxicity when amygdalin activation occurred specifically at tumor sites (Int J Cancer, PMID: 9833764). This was proof-of-concept for antibody-directed enzyme prodrug therapy (ADEPT) - a sophisticated targeting strategy largely abandoned despite its promise.
Cervical Cancer: Multiple studies have shown amygdalin-induced apoptosis in HeLa cells (the immortal cell line derived from Henrietta Lacks) via mitochondrial pathway activation. The same intrinsic apoptosis mechanisms observed in prostate cancer cells operate in cervical cancer.
Colorectal Cancer: Research documented cell viability reduction and increased apoptotic markers in HCT-116 and Caco-2 cell lines - common models for studying colorectal malignancies. Dose-dependent cytotoxicity was observed, with higher concentrations producing greater cell death.
Lung Cancer: Studies on A549 non-small cell lung cancer cells revealed dose-dependent cytotoxicity with minimal effects on normal bronchial epithelial cells. The therapeutic window - the difference between cancer-killing and normal-cell-killing doses - was measurable and significant.
Pancreatic Cancer: Though clinical evidence is limited, in vitro studies have documented amygdalin's effects on pancreatic cancer cell lines, which are notoriously resistant to conventional chemotherapy. Given pancreatic cancer's dismal prognosis and limited treatment options, any compound showing activity deserves investigation.
But they don't tell you about this breadth of research at oncology conferences. The conversation remains locked in the 1970s, frozen by institutional fear of challenging pharmaceutical industry interests and the regulatory status quo.
The Synergistic Potential: Combination Strategies
Fernandes & Billa (2025) reviewed combination strategies systematically: amygdalin with conventional chemotherapy, with immunotherapy checkpoint inhibitors, with other botanical compounds like curcumin and resveratrol (Biomed Pharmacother). The emerging picture suggests amygdalin may sensitize resistant cancers to standard treatments - making failed therapies work again by overcoming resistance mechanisms. While this paper was later retracted by the journal the authors dispute the retraction, see note in the references.
The research on cisplatin-resistant ovarian cancer cells is particularly striking. Amygdalin pre-treatment restored sensitivity to the platinum drug. Cells that had developed efflux pumps and DNA repair mechanisms to evade cisplatin became vulnerable again when exposed to amygdalin first. That's not alternative medicine competing with conventional treatment - that's adjuvant therapy that could extend lives and restore treatment options.
Similarly, studies have explored amygdalin combined with radiotherapy. Ionizing radiation works by generating reactive oxygen species (ROS) that damage DNA. Cancer cells often upregulate antioxidant defenses to survive radiation. Amygdalin appears to interfere with these adaptive responses, enhancing radiosensitivity.
The Tumor Microenvironment Factor
Recent research has moved beyond isolated cancer cells to examine amygdalin's effects on the tumor microenvironment - the complex ecosystem of immune cells, blood vessels, fibroblasts, and extracellular matrix that surrounds and supports tumors. it's a step in the right direction but not quite a full realization of the metabolic role in cancer.
Spanoudaki et al. (2023) reviewed evidence that amygdalin may modulate angiogenesis (blood vessel formation that feeds tumors) and immune cell infiltration. Tumors that can recruit blood vessels grow rapidly and metastasize. Tumors that can evade immune surveillance survive despite the body's defenses. Compounds that interfere with these processes attack cancer through mechanisms orthogonal to direct cytotoxicity.
The Anti-Inflammatory Connection
Chronic inflammation is increasingly recognized as a cancer promoter - creating an environment where cells accumulate mutations, evade immune elimination, and acquire invasive properties. Barakat et al. (2022) documented amygdalin's suppression of NF-κB (nuclear factor kappa B), the master transcriptional regulator of inflammatory gene expression.
When NF-κB is activated, it drives production of inflammatory cytokines like TNF-α, IL-1β, and IL-6 - all implicated in cancer progression. Suppressing NF-κB doesn't just reduce inflammation; it may slow cancer evolution and metastasis. Keep in mind, this is a systemic benefit that extends beyond direct tumor killing.
The Limitations We Must Acknowledge
Here's what the research also shows clearly: most of these studies are in vitro (cell culture) or in animal models. The clinical trial data in humans remains limited, often poorly designed, and methodologically flawed by modern standards. However the case histories have stacked up far beyond the hundreds of published case histories into the thousands online, and that's just the people talking about it risking censorship on youtube. We have compelling mechanistic evidence and promising preclinical data, but the bridge to validated clinical efficacy remains incomplete because it's the kryptonite of substances to study in cancer.
After all, it's extraordinarily difficult to conduct rigorous trials when the FDA won't approve them, institutional review boards are hostile, funding agencies won't support them, and pharmaceutical companies have no financial incentive to sponsor research on an unpatentable natural compound. The lack of human data isn't proof of inefficacy - it's proof of institutional and economic barriers to investigation.
What we have is mechanistically sound, biologically plausible, and preliminarily promising. What we need are properly designed phase II and III clinical trials with adequate sample sizes, appropriate patient selection, validated endpoints, and rigorous statistical analysis. But that requires acknowledgment that natural compounds deserve the same research investment as synthetic drugs - an acknowledgment the pharmaceutical industry fiercely resists.
The Shift Is Happening Whether They Like It Or Not
The research pipeline from 2021-2025 shows acceleration, not decline. Scientists are publishing in respected journals: Molecules, Cancers, International Journal of Molecular Sciences, Biomedicine & Pharmacotherapy, Scientific Reports, PLoS One. These aren't fringe publications run by alternative medicine advocates. These are peer-reviewed, indexed, mainstream scientific outlets with rigorous editorial standards.
Keep in mind, institutional resistance is crumbling under the weight of molecular evidence. Researchers in Germany, Greece, Egypt, Pakistan, and China are conducting studies that would be career suicide in American academic medicine. The globalization of science is breaking the FDA's monopoly on determining what gets investigated.
The question isn't whether amygdalin has anticancer activity. The research has answered that affirmatively across multiple cancer types and dozens of independent studies. The question is whether the medical establishment will allow that research to reach its full clinical potential, or whether economic interests will continue to suppress what can't be profitably patented.
After all, the truth doesn't require institutional approval. It just requires scientists courageous enough to follow the data wherever it leads.
References
1. Tsaur I, Makarević J, Hudak L, Juengel E, Kurosch M, Wiesner C, Bartsch G, Harder S, Haferkamp A, Blaheta RA. Amygdalin Exerts Antitumor Activity in Taxane-Resistant Prostate Cancer Cells. Cancers (Basel). 2022 Jun 23;14(13):3111. PMID: 35804883; PMCID: PMC9265127 . https://pubmed.ncbi.nlm.nih.gov/35804883/
2. Spanoudaki M, Stoumpou S, Papadopoulou SK, Karafyllaki D, Solovos E, Papadopoulos K, Giannakoula A, Giaginis C. Amygdalin as a Promising Anticancer Agent: Molecular Mechanisms and Future Perspectives. Int J Mol Sci. 2023 Sep 19;24(18):14270. PMID: 37762572; PMCID: PMC10531689 . https://pubmed.ncbi.nlm.nih.gov/37762572/
3. Barakat H, Aljutaily T, Almujaydil MS, Algheshairy RM, Alhomaid RM, Almutairi AS, Alshimali SI, Abdellatif AAH. Amygdalin: A Review on Its Characteristics, Antioxidant Potential, Gastrointestinal Microbiota Intervention, Anticancer Therapeutic and Mechanisms, Toxicity, and Encapsulation. Biomolecules. 2022 Oct 19;12(10):1514. PMID: 36291723; PMCID: PMC9599719. https://pubmed.ncbi.nlm.nih.gov/36291723/
4. Makarević J, Rutz J, Juengel E, Kaulfuss S, Reiter M, Tsaur I, Bartsch G, Haferkamp A, Blaheta RA. Amygdalin blocks bladder cancer cell growth in vitro by diminishing cyclin A and cdk2. PLoS One. 2014 Aug 19;9(8):e105590. PMID: 25136960; PMCID: PMC4138189 . https://pubmed.ncbi.nlm.nih.gov/25136960/
5. Makarević J, Rutz J, Juengel E, Kaulfuss S, Tsaur I, Nelson K, Pfitzenmaier J, Haferkamp A, Blaheta RA. Amygdalin influences bladder cancer cell adhesion and invasion in vitro. PLoS One. 2014 Oct 15;9(10):e110244. PMID: 25333694; PMCID: PMC4198254 . https://pubmed.ncbi.nlm.nih.gov/25333694/
6. Abdel-Mageid AD, Abou-Salem MES, Salaam NHA, El-Garhy HAS. Protective and chemotherapeutical role of amygdalin in induced mammary cancer. Sci Rep. 2025;15(1). (Early 2025 publication) https://pubmed.ncbi.nlm.nih.gov/40097629/
7. Fernandes RO, Billa N. Amygdalin in antineoplastic medicine and the relevance of nanotechnology. Biomed Pharmacother. 2025;182:117772. https://pubmed.ncbi.nlm.nih.gov/39700870/ While the above article was "retracted" here's the authors note: "The authors disagree with the retraction and dispute the grounds for it."
8. Syrigos KN, Rowlinson-Busza G, Epenetos AA. In vitro cytotoxicity following specific activation of amygdalin by beta-glucosidase conjugated to a bladder cancer-associated monoclonal antibody. Int J Cancer. 1998 Dec 9;78(6):712-9. PMID: 9833764. https://pubmed.ncbi.nlm.nih.gov/9833764/
9. Cipollone R, Ascenzi P, Visca P. Enzymatic detoxification of cyanide: clues from Pseudomonas aeruginosa Rhodanese. J Mol Microbiol Biotechnol. 2008;15(2-3):199-211. PMID: 18685272. https://pubmed.ncbi.nlm.nih.gov/18685272/
10. Shi J, Chen Q, Xu M, Xia Q, Zheng T, Teng J, Li M, Fan L. Recent updates and future perspectives about amygdalin as a potential anticancer agent: A review. Cancer Med. 2019 Jun;8(6):3004-3011. PMID: 31066207; PMCID: PMC6558459 . https://pubmed.ncbi.nlm.nih.gov/31066207/
|


0 Comments
Join the conversation
Be the first to comment
Share your thoughts above.