
The Double-Edged Scissors - CRISPR and the Rewriting of Life |
An investigative report examining CRISPR technology, its medical promise, military applications, and the ethical implications of humanity's ability to edit the human genome |
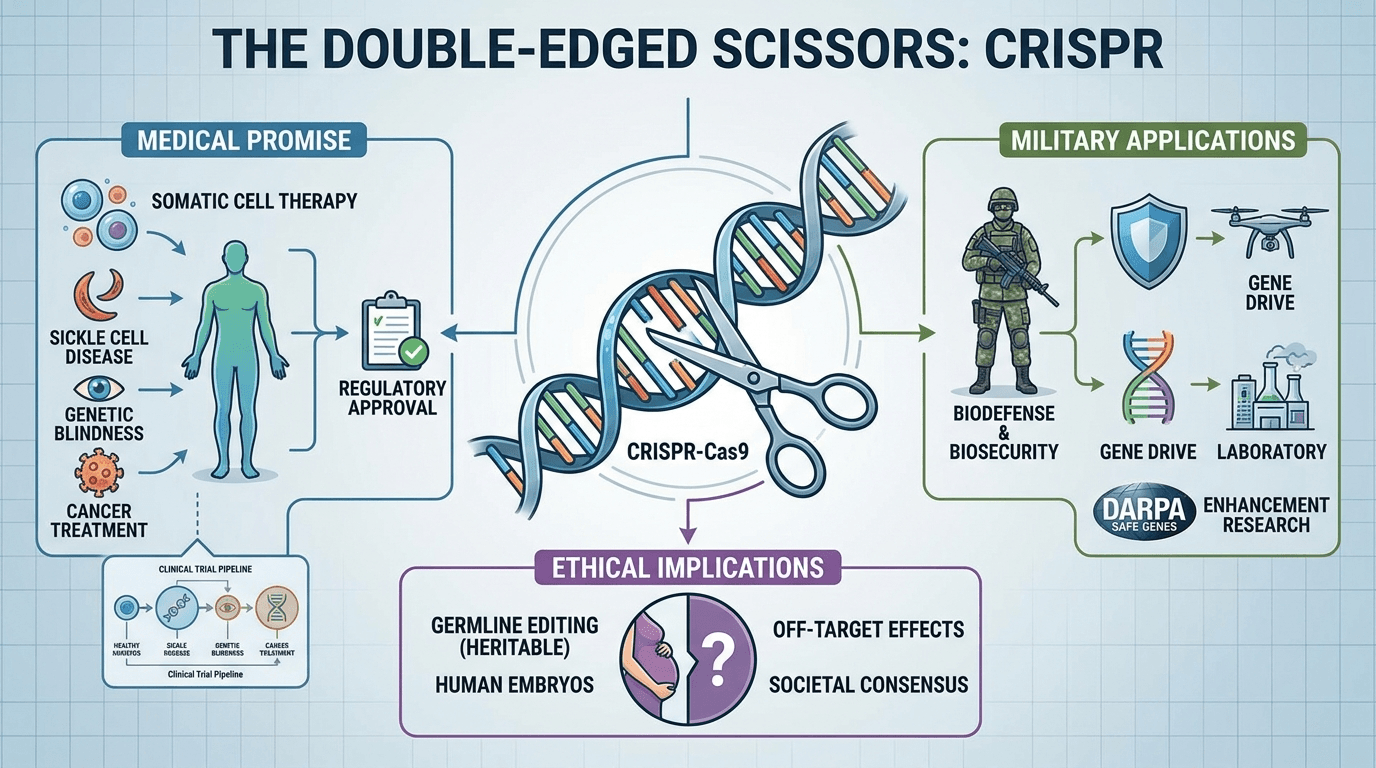
In 2012, a biological tool emerged from a seemingly obscure corner of microbiology research that would alter the trajectory of medicine, agriculture, and our understanding of life itself.
CRISPR-Cas9, adapted from the immune systems of bacteria, offered something scientists had long dreamed of: a precise, programmable way to rewrite the genetic code.
What began as a curiosity in the study of bacterial defense mechanisms has since evolved into a multi-billion-dollar industry racing to transform human health. But beneath the headlines celebrating its potential lies a far more complicated story, one that touches on military applications, germline editing, corporate power, and questions about what it means to intervene permanently in the human species.
From Bacteria to Breakthrough
The story of CRISPR begins not in a cutting-edge biotech laboratory but in the salt pools and hot springs where archaea and bacteria have been waging molecular warfare for billions of years.
These microorganisms evolved a defense mechanism against viruses: after surviving an infection, they would store fragments of the viral genetic code in their own DNA, forming a kind of molecular memory. When the virus attacked again, the bacteria could recognise it and deploy a protein called Cas9 to cut the invader's DNA apart.
In 2012, Martin Jinek and colleagues in Jennifer Doudna's laboratory at Berkeley, working in collaboration with Emmanuelle Charpentier's group, published the paper that would change everything.
They demonstrated that Cas9 could be programmed with a synthetic piece of RNA to cut DNA at any target sequence chosen by the researcher (Jinek et al., Science, 2012, PMID 22745249).
The implications were immediately understood: here was a molecular tool that could, in principle, edit any gene in any organism.
Within months, two independent research groups showed the system worked in human cells. Le Cong and colleagues at the Broad Institute demonstrated that CRISPR could precisely cut human DNA at multiple sites simultaneously (Cong et al., Science, 2013, PMID 23287718). Prashant Mali and colleagues in George Church's laboratory at Harvard confirmed the same capability, showing targeting rates of 10 to 25 per cent in human cell lines (Mali et al., Science, 2013, PMID 23287722). The technology had crossed the threshold from proof-of-concept to practical tool in the space of a single year.
Patrick Hsu, Eric Lander, and Feng Zhang subsequently published a comprehensive review of how CRISPR-Cas9 could be applied across research and medicine, laying out both its extraordinary possibilities and the challenges ahead (Hsu et al., Cell, 2014, PMID 24906146).
Jennifer Doudna's own 2014 Science review further cemented the framework, describing a "new era in which genomic manipulation is no longer a bottleneck to experiments" (Doudna et al., Science, 2014, PMID 25430774).
What made CRISPR so revolutionary was not simply its precision but its accessibility. Earlier gene-editing tools, such as zinc-finger nucleases and TALENs, required months of protein engineering for each new target. CRISPR required only a short RNA sequence that any molecular biology laboratory could synthesize cheaply. The cost of gene editing collapsed. The number of researchers able to use it exploded.
The Safety Questions That Arrived Quickly
The scientific community's enthusiasm was tempered almost immediately by a parallel set of concerns. Gene editing is only useful if the edits go where you intend them to go. Off-target cuts, where Cas9 mistakenly slices DNA at sequences that merely resemble the intended target, can introduce mutations that might do nothing, might be correctable, or might, in the wrong gene, contribute to cancer.
Early studies raised significant concerns. A 2017 report in Nature Methods (subsequently revised after methodological scrutiny) suggested that CRISPR editing in mice had produced hundreds of unintended mutations beyond the target site. The claim prompted heated debate: critics argued the mutations were pre-existing variants unrelated to CRISPR, and the paper was later substantially corrected.
The controversy itself was instructive. It demonstrated that the field's tools for detecting off-target effects were still maturing, and that the peer review process was being stress-tested by the technology's pace.
A more robust and lasting concern came in 2018. Michael Kosicki and colleagues at the Wellcome Sanger Institute published data showing that CRISPR cuts in mouse embryonic stem cells, mouse blood progenitor cells, and human cell lines frequently led not just to small insertions or deletions at the cut site but to large deletions spanning thousands of DNA base pairs, as well as complex chromosomal rearrangements (Kosicki et al., Nature Biotechnology, 2018, PMID 30010673).
These were structural changes that standard screening methods could miss entirely. The finding did not invalidate CRISPR therapy, but it established that the safety bar for clinical use needed to be set considerably higher than early optimism had suggested.
The Germline Crossing
No event in CRISPR's short history attracted more global attention or more uniform condemnation from the scientific community than the announcement made in November 2018 by He Jiankui, a Chinese biophysicist who revealed that he had used CRISPR to edit the embryos of human twins before birth.
He claimed to have disabled the CCR5 gene, which codes for a protein that HIV uses to enter immune cells, with the intention of making the children resistant to HIV infection. The twins, known publicly as Lulu and Nana, were born. A third CRISPR-edited pregnancy was reportedly underway.
The reaction from scientists and ethicists was swift and nearly unanimous in its criticism. The procedure was performed without adequate oversight, without the informed consent framework required for human subjects research, and on the basis of a claimed medical need (HIV prevention) for which far less drastic and well-established interventions already exist.
The edits were made to the germline: unlike somatic cell therapies, which alter the cells of a single individual, germline editing produces changes that will be passed to all future descendants. He was subsequently sentenced by Chinese courts to three years in prison (Cyranoski, Nature, 2019, PMID 30809070).
The incident crystallized a debate that scientists had been having more quietly since at least 2017. The National Academies of Sciences and Medicine had published a comprehensive report on human genome editing in 2017, concluding that germline editing should not proceed to clinical use until the technology was far better understood and broad societal consensus had been reached (National Academies, Human Genome Editing: Science, Ethics, and Governance, 2017, https://nap.nationalacademies.org/catalog/24623).
He Jiankui proceeded anyway.
The question of germline editing is not simply a question about one rogue scientist. It raises the prospect of heritable genetic changes becoming a permanent feature of certain human lineages. If editing embryos to eliminate a disease gene becomes technically safe and socially normalized, the line between treatment and enhancement becomes difficult to hold. Genes do not operate in isolation; most traits of interest, from intelligence to height to disease resistance, involve hundreds of variants, each with small effects. But the direction of travel is clear, and the ethical frameworks for governing it remain contested.
Medicine's New Frontier
While the germline controversy was still reverberating, CRISPR's clinical potential was advancing on a separate and less contested track: somatic cell therapy, where edits are made to the non-reproductive cells of a living patient and do not pass to descendants.
The results have been striking. In 2021, researchers from Intellia Therapeutics published the first evidence of successful in vivo CRISPR editing in humans: a clinical trial targeting the gene responsible for producing a misfolded protein called transthyretin, which accumulates in the nerves and heart of patients with hereditary transthyretin amyloidosis. A single infusion of CRISPR machinery inside lipid nanoparticles reduced blood levels of the toxic protein by up to 87 per cent (Gillmore et al., NEJM, 2021, PMID 34215024).
This was CRISPR working inside the body, navigating to the liver, entering cells, and making targeted cuts in living human tissue.
That same year, Haydar Frangoul and colleagues published trial data on CTX001 (later branded exa-cel) for sickle cell disease and beta-thalassaemia. The approach used CRISPR to reactivate foetal haemoglobin in patients' own blood stem cells, effectively switching back on a genetic program that is normally silenced after birth. Early results showed patients becoming transfusion-independent (Frangoul et al., NEJM, 2021, PMID 33283989).
In December 2023, the US Food and Drug Administration approved exagamglogene autotemcel (Casgevy) for the treatment of sickle cell disease in patients aged 12 and over: the first CRISPR-based therapy to receive regulatory approval anywhere in the world (FDA press release, 8 December 2023). The approval was a threshold moment. Gene editing had moved from laboratory to licensed medicine in just over a decade.
The pipeline behind Casgevy is extensive. Clinical trials are underway for CRISPR-based treatments targeting HIV, certain cancers, Duchenne muscular dystrophy, and multiple inherited blindness disorders. Each presents a different set of delivery challenges (getting the editing machinery into the right cells) and a different safety profile. The field is not moving at a single speed; each disease application is its own engineering problem.
The Military Dimension
Less visible in the mainstream narrative around CRISPR but no less significant is the attention the technology has attracted from defense establishments.
In 2016, the United States Defense Advanced Research Projects Agency launched its Safe Genes program, committing tens of millions of dollars to research into the control, containment, and reversal of gene editing.
The stated rationale was defensive: protecting military personnel from accidental or intentional misuse of genome editing technologies, and developing "genetic remediation" strategies to undo unwanted edits in biological systems (DARPA, Safe Genes program, https://www.darpa.mil/research/programs/safe-genes). The framing was protective. But the same research that builds a lock also builds a key.
DARPA's interest in gene editing cannot be cleanly separated from questions about human enhancement. If CRISPR can eliminate a disease gene, it can, in principle, also amplify a performance trait: oxygen efficiency, pain tolerance, sleep requirement. These applications may be years or decades away from practicality, and enormous scientific hurdles remain. But that direction of travel was not accidental in DARPA's portfolio, and several government and independent bodies have examined its implications.
The National Academies' 2018 report on biodefense in the age of synthetic biology was explicit that gene editing technologies, including CRISPR, posed novel challenges for national security (National Academies, Biodefense in the Age of Synthetic Biology, 2018, https://nap.nationalacademies.org/catalog/24890).
The concern is not merely that states might pursue enhancement programs. It is that gene-drive technologies, which use CRISPR to spread specific edits through entire wild populations of insects or rodents, could be weaponized to devastate agricultural systems or engineer disease vectors.
This is not a science fiction scenario; gene drives have been demonstrated in laboratory settings and field trials are under discussion for malaria control.
What Governance Can Do
The standard response to concern about emerging biotechnologies is to call for regulation. In the case of CRISPR, the call has been answered with a patchwork.
The International Commission on the Clinical Use of Human Germline Genome Editing, convened jointly by the US National Academies and the UK's Royal Society, concluded in 2020 that heritable human genome editing should not proceed in any country until it could be done safely and until robust oversight systems were in place.
Most major research jurisdictions prohibit clinical germline editing. China tightened its regulations following the He Jiankui case. But the world is large, and regulatory arbitrage remains a real possibility: what is prohibited in one jurisdiction can simply be attempted in another.
The deeper governance challenge is that CRISPR's most powerful applications are not controlled by a handful of large institutions. The technology is genuinely accessible. A competent molecular biologist with a few thousand pounds of equipment can perform CRISPR experiments. The tools are described in published literature, the reagents are commercially available, and the guides for any target sequence can be designed with free online software.
This has democratized biological research in ways that are overwhelmingly beneficial. It also makes comprehensive oversight structurally difficult in a way that nuclear or chemical weapons programs are not.
The comparison with previous transformative biotechnologies is instructive. Recombinant DNA technology, first demonstrated in the early 1970s, prompted the Asilomar Conference of 1975, in which scientists voluntarily paused certain experiments and agreed to biosafety protocols while governance frameworks caught up.
CRISPR has not had its Asilomar moment, partly because the technology moved faster than any moratorium could have contained, and partly because the applications are too numerous and distributed for a single pause to be meaningful.
The Commercial Architecture
Behind the scientific debates sits a substantial commercial infrastructure. CRISPR has generated several multi-billion-dollar companies, most notably Editas Medicine, CRISPR Therapeutics, and Intellia Therapeutics, each with distinct technology platforms and patent positions.
The patent dispute over foundational CRISPR intellectual property, fought between teams led by Jennifer Doudna at Berkeley and Feng Zhang at the Broad Institute, lasted for years and resulted in a complex allocation of rights that has shaped who can commercialize what in different therapeutic contexts.
The commercial pressure cuts both ways. On one hand, it has accelerated clinical development; companies with significant investment have every incentive to move quickly through trials. On the other, it creates tension around data transparency, access to therapies, and the prioritization of diseases that affect wealthy populations over those that primarily afflict the global poor.
Sickle cell disease, despite being among the first conditions to receive an approved CRISPR treatment, disproportionately affects people of African descent; the price of Casgevy at launch was reported at approximately over $2 million per patient in the US market. The gap between what the technology can do and who can access it is not a technical problem.
The Longer View
CRISPR has been in clinical development for less than a decade. The cells in the human body divide, repair themselves, and interact with their environment across a lifetime. The long-term consequences of CRISPR edits in somatic tissues, particularly edits made during childhood, are not yet known because the children who received early treatments have not yet lived long enough for that data to exist. This is not a reason to halt development, but it is a reason for the confidence intervals around claims of safety to remain wide.
The genuine achievements are substantial. A therapy that can free a patient with sickle cell disease from a lifetime of crises and transfusions is a meaningful medical advance. An in vivo gene edit that reduces a toxic protein by nearly 90 per cent in a single infusion is extraordinary pharmacology. The basic science that made these possible, from understanding bacterial immunity to engineering guide RNAs, represents one of the most productive decades in the history of molecular biology.
The concerns are also real. Off-target effects remain an active area of research rather than a solved problem. The germline boundary, once crossed, cannot be uncrossed for the lineages that carry the edit. The potential for dual-use applications in defense contexts is not theoretical. And the governance frameworks adequate to the technology's reach do not yet exist.
CRISPR is neither the salvation its most optimistic proponents describe nor the catastrophe its most alarmed critics fear. It is a tool of extraordinary power in the hands of researchers who are flawed human beings, often striving for more power through science. We can't assume these are honorable humans with good intentions, nor can we assume the institutions they represent are truly honorable.
Personally I see this through a lens of eugenicist corruption and have major concerns about this technology and what may be going on in secretive labs in unnamed jurisdictions. Without a clear understanding of the history of eugenics, it's difficult to understand what sort of intentions the top scientists of CRISPR may actually be aiming for.
The scissors are real. So is the edge on both sides, and it's sharper than you might think.
Share your thoughts in the comments below.
References
|

5 Comments
Join the conversation
Genuinely didn't know DARPA had a whole program funding CRISPR research since 2016. The framing of it as purely defensive is doing a lot of heavy lifting there. Build tools to reverse gene edits... which means you also understand exactly how to make them irreversible. Not reassuring.
Thank you for bringing up the eugenics history angle at the end. Most of these articles skip right past it. The scientists who built the early eugenics movement also believed they were doing something beneficial for humanity. That context doesn't just disappear because the tools are more precise now.
I work in a molecular biology lab (not on CRISPR specifically) and the bit about accessibility is completely true. The barrier to entry dropped dramatically. That's exciting for legitimate research but it does make you think about what's happening in places with no oversight at all.
$2 million per patient for Casgevy. Sickle cell predominantly affects people of African descent. And somehow we're supposed to celebrate this as a breakthrough for humanity? The breakthrough exists. The access does not. Those are two very different things.
The part about He Jiankui just sat with me. Three years in prison for editing the germline of actual human beings who now have to live with whatever was done to them. And we still don't fully know what the long-term effects are for those children. That's what keeps me up at night about all this.