
The Microbiome Connection: How Gut Bacteria Unlock Amygdalin's Potential |
Enter Subtitle |
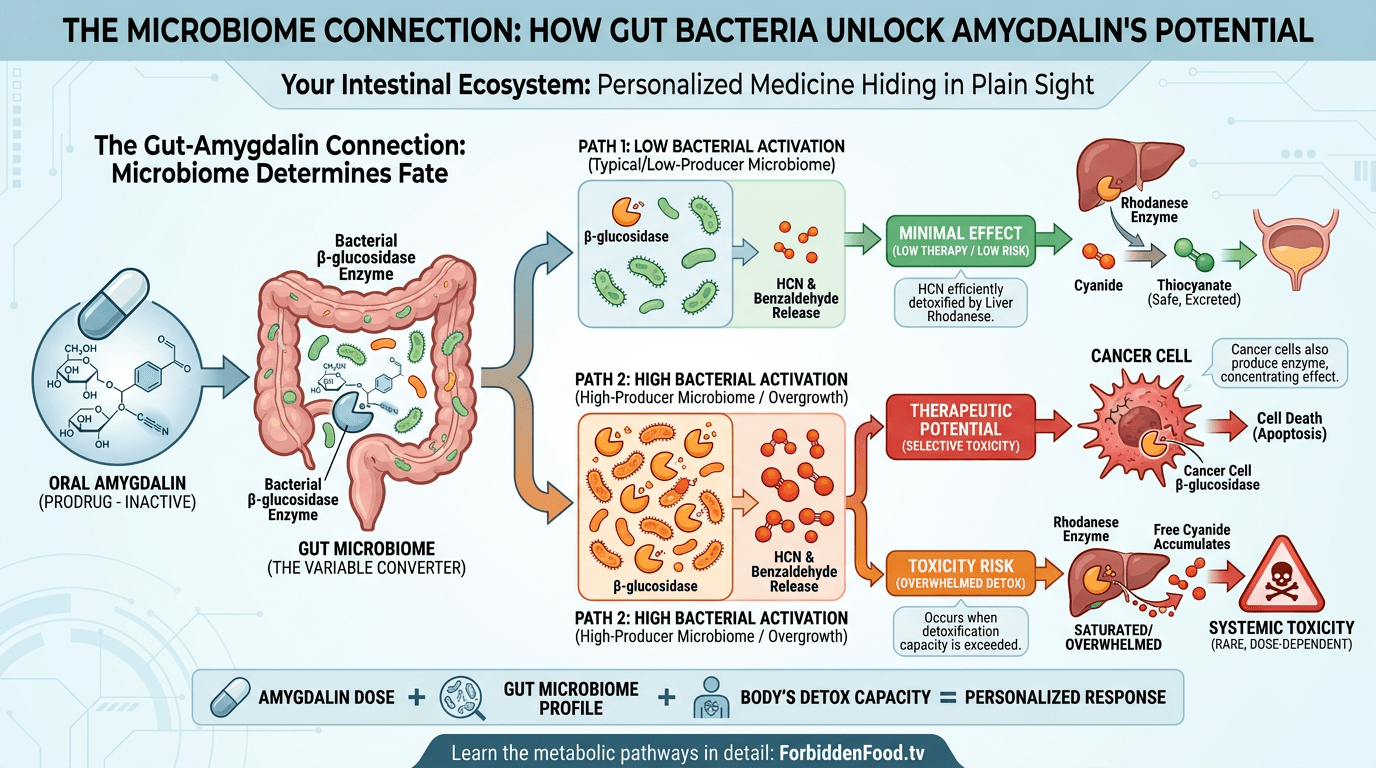
Your gut bacteria might hold the key to unlocking amygdalin's therapeutic potential - or its toxic risk. But they don't tell you that the difference between poison and medicine may come down entirely to which microbial species are colonizing your intestines, metabolizing your food, and producing the enzymes that activate or detoxify natural compounds.
After all, amygdalin doesn't work in isolation. It's a prodrug - an inactive precursor requiring metabolic conversion to become active. And that transformation depends critically on an enzyme, beta-glucosidase, produced not by your human cells but by cancer cells, and in small amounts potentially by your gut microbiota. You're not just treating a human - you're treating a superorganism composed of human cells plus trillions of bacterial partners.
The Bacterial Enzyme That Changes Everything
Amygdalin is a prodrug in the truest sense: biologically inactive until cleaved by specific enzymes. When you consume amygdalin orally - whether from apricot kernels, bitter almonds, or pharmaceutical preparations - it passes through your stomach largely intact, protected by its glycosidic bonds from acid hydrolysis. The real transformation happens in the intestines, where bacterial metabolism takes over.
Specific bacterial species produce beta-glucosidase, the enzyme that cleaves amygdalin's glycosidic bonds sequentially: first removing one glucose unit to form prunasin, then cleaving the second glucose to release benzaldehyde and hydrogen cyanide. The key species include Lactobacillus strains (particularly L. plantarum and L. rhamnosus), Bifidobacterium species (B. longum, B. adolescentis), Bacteroides species, and certain Clostridium strains.
Barakat et al. (2022) documented this microbial partnership in extensive detail (PMC9599719). The composition of your gut microbiome - which varies dramatically between individuals based on diet, geography, antibiotic exposure, and genetics - determines how much amygdalin gets activated, how quickly activation occurs, and where in the GI tract the process happens.
Here's the rub: people with radically different gut bacterial profiles will respond completely differently to the same dose of amygdalin. It's personalized medicine by accident - your microbes are effectively titrating your dose based on their enzymatic capacity. Someone with high Lactobacillus counts might activate amygdalin rapidly and extensively, potentially approaching toxic thresholds, but the toxic effects are largely overblown in media reports as a scare tactic. In fact we have redundant mechanisms of removing these compounds from the body. Someone with low beta-glucosidase-producing species might activate very little, experiencing minimal therapeutic effect or toxicity but I go into more detail on the specific metabolic pathways in the free online course at https://ForbiddenFood.tv
The Hydrogen Cyanide Release Paradox
Critics obsess over hydrogen cyanide as if the mere presence of HCN equals inevitable poisoning. Proponents argue it's precisely the mechanism of therapeutic selectivity. The truth lies in the dose-response relationship and the body's detoxification capacity.
Keep in mind, the dose makes the poison - a principle established by Paracelsus in the 16th century. Small amounts of HCN released gradually in the intestines can be efficiently detoxified by rhodanese (thiosulfate sulfurtransferase), an enzyme abundant in liver and kidney mitochondria that converts cyanide to thiocyanate. Thiocyanate is far less toxic and is readily excreted in urine.
Cipollone et al. (2006) demonstrated that recombinant rhodanese can effectively detoxify environmental cyanide, and Luo et al. (2025) recently reviewed the therapeutic potential of enhancing thiosulfate sulfurtransferase activity for protection against toxic exposures (Redox Biol, PMID: 40107018).
But when beta-glucosidase activity is excessively high - whether from bacterial overgrowth, specific high-producer strains, or consumption of very high amygdalin doses - HCN release can overwhelm rhodanese capacity. The detoxification system becomes saturated. Free cyanide accumulates. Toxicity occurs, however this is quite rare due to typical low conversion rates or only high conversion in cancer cells.
After all, the therapeutic window isn't determined solely by the amygdalin dose. It's a three-way interaction between amygdalin intake, gut bacterial beta-glucosidase activity, cancer cell beta-glucosidase activity and hepatic rhodanese detoxification capacity. Four variables, not one. This complexity explains why traditional dosing guidelines based purely on milligrams of amygdalin are inadequate.
Microbiome Variation Explains Clinical Inconsistency
One of the most devastating criticisms of historical laetrile studies was wildly inconsistent patient responses. In the same trial, some patients reported subjective benefits and tumor responses. Others experienced severe toxicity including cyanide poisoning, though it can be argued this was largely the result of intentionally flawed study design to crush amygdalin in favor of pharma controlled molecules. Clinical trials showed contradictory results that couldn't be reconciled, and often couldn't be replicated.
But they don't tell you that none of those studies - not the Moertel trial, not the earlier case series, not the Mexican clinic reports - assessed gut microbiome composition. This was decades before the Human Microbiome Project, before we understood that microbial profiles vary more dramatically between individuals than human genetics do.
Two genetically identical twins can have radically different gut microbiomes based on diet, antibiotic exposure, and environmental factors. Two people taking identical amygdalin doses might experience completely different enzymatic conversion rates based solely on their bacterial populations, nevermind the cancer cell load. Without microbiome analysis, early studies were essentially flying blind, unable to explain why Patient A tolerated treatment while Patient B suffered toxicity.
Keep in mind, this isn't a historical curiosity - it's a fundamental challenge for any orally administered prodrug that depends on bacterial activation. The solution isn't abandoning the compound; it's implementing microbiome-guided precision dosing.
Also keep in mind that much of the early research was centered around intravenous injection of the amygdalin and when studies were designed properly these consistently showed promise in positive anecdotal response as well as promising unpublished mouse studies from Dr Harold Manner which are covered in my free course at https://ForbiddenFood.tv
The Probiotic Strategy: Standardizing the Unstandardizable
Spanoudaki et al. (2023) explored a fascinating therapeutic angle: could probiotic supplementation optimize amygdalin's effects by modulating gut bacterial composition (PMID: 37762572)?
Certain probiotic strains produce moderate, controlled levels of beta-glucosidase - enough to activate amygdalin gradually and safely, but not enough to cause rapid, overwhelming cyanide release. Supplementing with these specific strains before and during amygdalin therapy could theoretically standardize metabolic conversion, reducing inter-individual variability.
Promising strains include:
• Lactobacillus plantarum: Produces moderate beta-glucosidase, well-tolerated, already used in commercial probiotics for digestive health.
The strategy would involve probiotic pretreatment for 2-4 weeks to establish stable colonization, followed by gradual amygdalin introduction with close monitoring. The probiotics effectively "prime" the gut environment for controlled amygdalin activation.
This isn't wild speculation - it's microbiome pharmacology, an emerging field recognizing that our bacterial passengers are active participants in drug metabolism, not passive bystanders. After all, the same principle applies to digoxin (metabolized by Eggerthella lenta), levodopa (decarboxylated by gut bacteria), and numerous other medications.
Nanotechnology: Bypassing Bacterial Variability Entirely
Here's where the research gets truly innovative: if bacterial metabolism is inherently unpredictable and variable, why not engineer delivery systems that control amygdalin release independent of gut microbes?
Fernandes & Billa (2025) reviewed nanoparticle formulations designed to target specific tissues - particularly tumors - while minimizing systemic exposure and unpredictable bacterial degradation in the gut (Biomed Pharmacother).
Alginate-Chitosan Nanoparticles (ACNPs): Sohail et al. (2020) synthesized and characterized amygdalin-loaded ACNPs, demonstrating that these biodegradable polymer nanoparticles encapsulate amygdalin, protecting it during transit through the stomach and upper GI tract (Int J Biol Macromol, PMID: 32097740). Release occurs in response to pH changes or specific enzymatic environments - like the acidic, enzyme-rich tumor microenvironment.
The advantages are transformative:
• Reduced gut bacterial activation: Encapsulated amygdalin bypasses intestinal beta-glucosidase, dramatically lowering systemic cyanide exposure from GI metabolism, however theoretic the high rates of conversion may be.
Prajapati et al. (2025) reviewed recent trends in nanoparticulate delivery systems for amygdalin, documenting the explosion of innovation in this space (Curr Drug Deliv, PMID: 38037911).
Additional Nanoformulation Strategies
Carboxymethyl Chitosan Nanoparticles: El-Houssiny et al. (2024) assessed cytotoxic effects of CMC-NP-loaded amygdalin against cancer vs. normal cell lines, demonstrating selective toxicity enhancement (Discov Nano, PMID: 38573410). The nanoformulation killed cancer cells at lower concentrations than free amygdalin while showing reduced toxicity to normal cells - the holy grail of oncology therapeutics.
Targeted Nanocomposite Systems: Baghdady et al. (2026) developed a sophisticated chitosan/reduced graphene oxide-zinc oxide/hyaluronic acid nanocomposite specifically for head and neck squamous cell carcinoma (BMC Oral Health, PMID: 41882653). Hyaluronic acid targets CD44 receptors overexpressed on cancer cells, enabling active rather than passive targeting.
Liposomal Encapsulation: Lipid vesicles that fuse directly with cell membranes, delivering amygdalin into the cytoplasm while bypassing bacterial enzymes entirely. Extended circulation time allows accumulation at tumor sites.
PEGylated Nanoparticles: Polyethylene glycol coating creates a "stealth" effect, preventing immune clearance and extending circulation time. Amygdalin can reach distant metastases before degradation.
Magnetic Nanoparticles: Iron oxide particles loaded with amygdalin that can be guided to specific body regions using external magnetic fields. This enables literal remote control of drug delivery - science fiction becoming therapeutic reality.
Keep in mind, these aren't theoretical proposals. These are published, peer-reviewed studies with in vitro and in vivo validation. The technology exists now to overcome the gut microbiome variability problem entirely.
The Tumor Microbiome Factor: Cancer's Bacterial Passengers
Recent microbiome research has revealed something remarkable and slightly unsettling: tumors have their own microbiomes. Pancreatic tumors, breast tumors, colon tumors - all harbor specific bacterial populations within the tumor tissue itself, not just in the surrounding environment.
If those intratumoral bacteria produce beta-glucosidase, amygdalin could be preferentially activated inside tumors - exactly where cytotoxic effects are desired. It's the original Trojan horse strategy, now potentially enhanced by microbial accomplices already residing inside the cancer.
We've known this effect for decades, now the microbiome research confirms the mechanisms involved in cancer cells producing 1000x or more concentration of beta-glucosidase.
Pancreatic cancers, notoriously resistant to conventional chemotherapy with dismal 5-year survival rates, often have unique bacterial signatures including Fusobacterium and Gammaproteobacteria species. Some of these produce glycosidases. Could amygdalin, delivered via nanoparticles to pancreatic tumors, be activated by the tumor's own microbiome? Could tumor microbiome profiling predict which cancers will respond best to amygdalin therapy?
After all, in the clinical research realm we're just beginning to understand that tumors aren't purely human tissue - they're complex ecosystems containing bacteria, fungi, and viruses that influence cancer behavior, treatment response, and prognosis. Exploiting this microbial component therapeutically represents a paradigm shift in oncology.
This research is well known to "shift" quite slowly due to pharma biases and a refusal to fully investigate the metabolic theories of cancer
The Clinical Translation Challenge: Science vs. Regulation
Here's what might make scientific and clinical sense for anyone that doesn't want to look at the hundreds of published case histories of taking amygdalin in high doses and want to rely on published studies:
1. Screen patients' gut microbiomes before amygdalin therapy using 16S rRNA sequencing to quantify beta-glucosidase-producing species.
Here's what actually happens clinically under current regulatory frameworks: none of this. Because amygdalin remains institutionally taboo despite mounting mechanistic evidence. Because microbiome-guided precision medicine for natural compounds doesn't fit the pharmaceutical industry business model. Because nanoformulation development requires investment that companies won't make for unpatentable molecules.
But they don't tell you that the barrier isn't scientific - it's political, regulatory, and economic. The tools exist. The knowledge exists. The technology exists. What's missing is institutional will and economic incentive to implement what science has already made possible.
The Personalized Medicine Future Hiding in Bitter Seeds
This article could easily conclude that amygdalin therapy exemplifies why one-size-fits-all medicine fails and why the future must be personalized and that therapeutic response depends on individual biological variation - not just in human genes but in microbial genes, not just in tumor cells but in tumor ecosystems.
However, I believe this to be misguided because all of this is simply an attempt to fix what's not broken.
After all, even while you're not treating a human in isolation. You're treating a superorganism - a human host plus trillions of bacteria, fungi, and viruses that metabolize, activate, detoxify, and modulate whatever compounds you ingest. Medicine that ignores this reality will continue producing inconsistent results and unexplained toxicities.
However, with amygdalin the metabolic outcomes are quite predictable and have much lower toxicity than what pharma biased doctors often promote.
The future of amygdalin isn't just better clinical trials, though we desperately need those. It may also include microbiome-aware, nanoformulated, tumor-targeted, personalized therapeutic strategies that work with biological complexity rather than pretending it doesn't exist.
Keep in mind, the patients who traveled to Mexican clinics in the 1970s seeking laetrile therapy weren't crazy or gullible. They were desperately seeking options when conventional medicine had failed them. It was rare for them to experience toxicity because it was largely delivered intravenously allowing incredibly high doses while minimizing toxic effect. Many reported benefits and many lives were saved.
Now we come back to oral dosing of amygdalin, which has been practiced consistently for decades with very little toxic effects.
Microbiome research on amygdalin is quite interesting, it's again important to understand that this trend towards individualized, microbiome tailored therapy is clearly popular in studies, but is it largely fixing a problem that was only broken by censorship and propaganda?
We're still waiting for "science" to catch up to the reason that amygdalin was so popular it couldn't even be stopped by outrageous state restrictions in the 1970s. It just flat out worked and people knew it!
Learn more about the metabolic benefits of apricot seed amygdalin and other nitriloside compounds in my free online course at https://ForbiddenFood.tv and try our seeds at https://EatApricotSeeds.com
References
1. Barakat H, Aljutaily T, Almujaydil MS, Algheshairy RM, Alhomaid RM, Almutairi AS, Alshimali SI, Abdellatif AAH. Amygdalin: Gastrointestinal Microbiota Intervention. Biomolecules. 2022 Oct 19;12(10):1514. PMID: 36291723; PMCID: PMC9599719. https://pubmed.ncbi.nlm.nih.gov/36291723/ 2. Spanoudaki M, Stoumpou S, Papadopoulou SK, Karafyllaki D, Solovos E, Papadopoulos K, Giannakoula A, Giaginis C. Future Perspectives for Development of Nanoformulations for Amygdalin Delivery. Int J Mol Sci. 2023 Sep 19;24(18):14270. PMID: 37762572; PMCID:PMC10531689 https://pubmed.ncbi.nlm.nih.gov/37762572/
3. Fernandes RO, Billa N. Amygdalin in antineoplastic medicine and the relevance of nanotechnology. Biomed Pharmacother. 2025;182:117772. https://pubmed.ncbi.nlm.nih.gov/39700870/ 4. Sohail R, Mathew M, Patel KK, Reddy SA, Haider Z, Naria M, Misra M, Kaul K. Evaluation of amygdalin-loaded alginate-chitosan nanoparticles as biocompatible drug delivery carriers for anticancerous efficacy. Int J Biol Macromol. 2020 Jun 15;153:36-45. PMID: 32097740. https://pubmed.ncbi.nlm.nih.gov/32097740/ 5. Prajapati M, Deshmukh R, Harwansh RK. Recent Trends in Nanoparticulate Delivery System for Amygdalin as Potential Therapeutic Herbal Bioactive Agent for Cancer Treatment. Curr Drug Deliv. 2025;22(1):63-79. PMID: 38037911. https://pubmed.ncbi.nlm.nih.gov/38037911/ 6. El-Houssiny AS, Soliman AAF, Abdel-Nour KN. Assessment of the cytotoxic effect of carboxymethyl chitosan-loaded amygdalin nanoparticles against human normal and cancer cell lines. Discov Nano. 2024 Apr 4;19(1):62. PMID: 38573410. https://pubmed.ncbi.nlm.nih.gov/38573410/ 7. Baghdady SI, Sabra SA, Darwish AB, Salama A, Kamoun EA, Hanafy SA. Targeted nanocomposite delivery system of amygdalin using chitosan/reduced graphene oxide-zinc oxide/hyaluronic acid for treatment of head and neck squamous cell carcinoma. BMC Oral Health. 2026 Mar 25;26(1):627. PMID: 41882653. https://pubmed.ncbi.nlm.nih.gov/41882653/ 8. Cipollone R, Ascenzi P, Frangipani E, Visca P. Cyanide detoxification by recombinant bacterial rhodanese. Chemosphere. 2006 May;63(6):942-9. PMID: 16307778. https://pubmed.ncbi.nlm.nih.gov/16307778/ 9. Luo Y, Melhem S, Feelisch M, Chatre L, Morton NM, Dolga AM, van Goor H. Thiosulphate sulfurtransferase: Biological roles and therapeutic potential. Redox Biol. 2025 May;82:103595. PMID: 40107018. https://pubmed.ncbi.nlm.nih.gov/40107018/ 10. Tumor Microbiome: Geller LT, Barzily-Rokni M, Danino T, et al. (2017). "Potential role of intratumor bacteria in mediating tumor resistance to the chemotherapeutic drug gemcitabine." Science, 357(6356):1156-1160. https://pubmed.ncbi.nlm.nih.gov/28912244/
|

0 Comments
Join the conversation
Be the first to comment
Share your thoughts above.